The Genesis of a Crisis: Tracing the Ebola Virus Outbreak's Origins
The year 2014 cast a dark shadow over West Africa, as the world witnessed the largest and most devastating outbreak of Ebola virus disease (EVD) in recorded history. This unprecedented epidemic, also known as Ebola hemorrhagic fever (EHF), originated in a remote corner of Guinea, unfolding with a tragic swiftness that caught global health authorities off guard. The first flicker of the impending crisis was traced back to December 2013, when a two-year-old child in the village of Meliandou, Guéckédou Prefecture, succumbed to a mysterious illness. This young life, tragically, became the index case of an outbreak that would eventually claim thousands.
The initial transmission of the Ebola virus to humans is believed to have been a zoonotic spillover event, a common characteristic of this formidable pathogen. Scientific investigations suggest that contact with infected fruit bats or non-human primates, likely through hunting and the consumption of bushmeat, facilitated the virus's leap across species. These animals serve as natural reservoirs for the Ebola virus, harboring it without displaying symptoms, yet capable of transmitting it to others. Once the virus entered the human population, its highly contagious nature, combined with a lack of awareness and inadequate public health infrastructure, set the stage for its rapid proliferation.
Ebola is a severe, often fatal, viral hemorrhagic fever. Its initial symptoms can be deceptively flu-like, including fever, intense weakness, muscle pain, headache, and a sore throat. As the disease progresses, patients typically develop vomiting, diarrhea, rash, and impaired kidney and liver function. In some cases, internal and external bleeding can occur, leading to a grim prognosis. The challenge of identifying and containing such a rapidly escalating threat in resource-limited settings proved immense, allowing the Ebola virus to gain a foothold before the world truly understood the gravity of the situation.
Unprecedented Spread: How Ebola Swept Across West Africa and Beyond
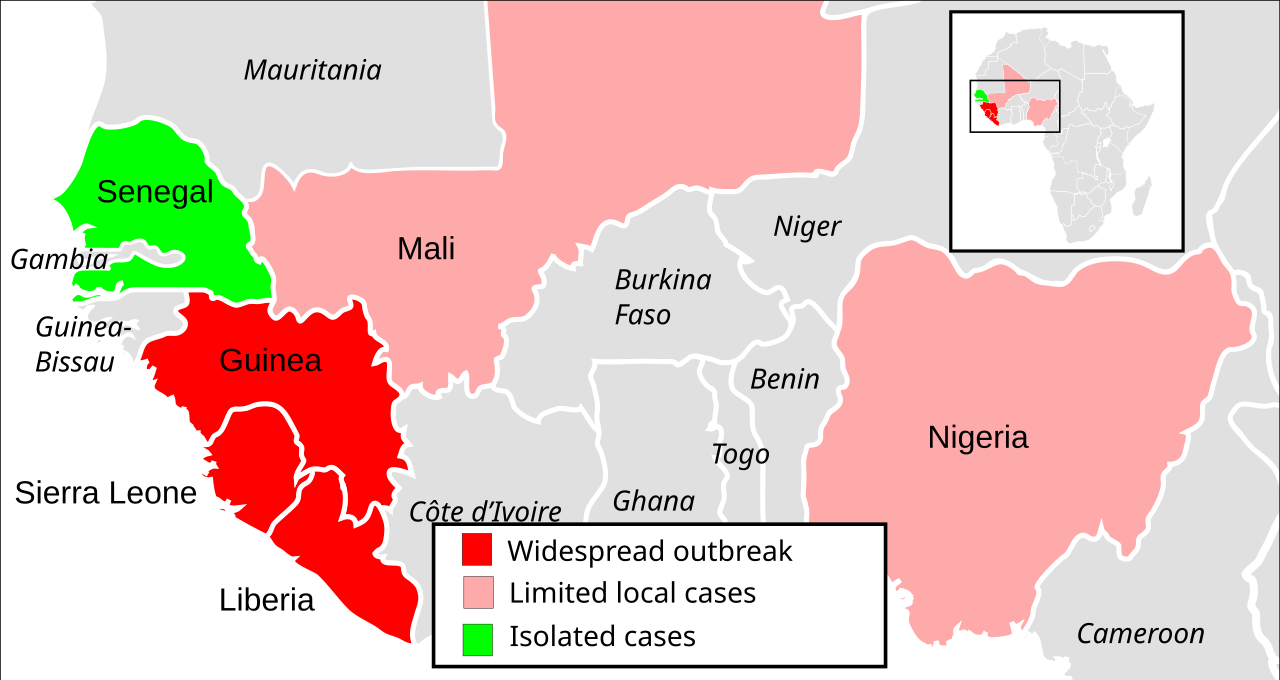
From its humble origins in Guinea, the Ebola virus swiftly breached borders. By late March 2014, cases had spread to neighboring Liberia and Sierra Leone, largely facilitated by cross-border travel, family contacts, and traditional burial practices that involve close physical contact with the deceased. The interconnectedness of communities in the region, coupled with initial delays in diagnosis and contact tracing, transformed what might have been a localized outbreak into a full-blown epidemic.
The characteristics of the affected regions—weak healthcare systems, limited laboratory capacity, and a general lack of trust in governmental responses—created fertile ground for the virus's unchecked spread. Healthcare workers, often ill-equipped and unprepared, became particularly vulnerable, with many contracting the disease while caring for patients. This not only exacerbated the crisis but also decimated already fragile medical workforces, further crippling the ability to mount an effective response.
The epidemic reached its peak in 2014-2015, ultimately infecting over 28,600 individuals and causing a staggering 11,325 deaths by June 2016. The sheer scale and duration of the West African crisis marked it as the largest Ebola outbreak ever recorded, dwarfing all previous incidents. While Guinea, Liberia, and Sierra Leone bore the brunt of the epidemic, the Ebola virus also made headlines globally when a traveler from Liberia arrived in Lagos in July 2014, resulting in 20 cases in Nigeria. This incident highlighted the potential for international spread and galvanized a more robust global response.
Factors Amplifying Transmission:
- Inadequate Contact Tracing: The inability to swiftly identify and monitor individuals who had come into contact with infected persons allowed the chain of transmission to continue largely unbroken.
- Limited Laboratory Capacity: Delays in testing and confirmation meant that infected individuals often went undiagnosed for critical periods, contributing to further spread.
- Cultural Practices: Traditional burial rites and caregiving customs, which involve close contact with bodily fluids, inadvertently amplified transmission.
- Weak Health Systems: Shortages of personnel, personal protective equipment (PPE), and isolation facilities overwhelmed local healthcare infrastructure.
- Lack of Public Trust: Misinformation and fear often led to communities resisting public health interventions, making containment efforts challenging.
The Ebola Virus Reaches New Shores: Cases in the United States and Global Preparedness
The 2014 West African Ebola epidemic was not confined to Africa; it also tested the preparedness of nations far removed from the epicentre. The United States, for instance, saw eleven individuals treated for confirmed Ebola virus disease infections between 2014 and 2016. All these cases were directly linked to the West African outbreak, revealing both vulnerabilities and strengths in the US public health system.
The most prominent case involved Thomas Eric Duncan, an index patient who acquired the infection abroad and traveled to Texas. His hospitalization at Texas Presbyterian Hospital unfortunately led to two secondary transmissions to healthcare workers in Dallas. These transmissions were attributed to breaches in personal protective equipment (PPE) protocols during his care, exposing critical gaps in the initial response capabilities of even advanced healthcare settings. Tragically, Mr. Duncan succumbed to the disease on October 8, 2014. Another physician, infected abroad and evacuated to the US, also deteriorated despite advanced supportive care and ultimately died.
The remaining patients treated in the US were primarily medical personnel or missionaries who had contracted the virus in affected West African regions. They were safely evacuated and received specialized care in state-of-the-art biocontainment units at facilities such as the NIH Clinical Center in Maryland and Emory University Hospital in Georgia. This demonstrated the vital role of specialized units and advanced supportive care in managing severe EVD cases. Crucially, no further domestic transmissions occurred beyond the Dallas cluster, a testament to the effectiveness of enhanced infection control measures implemented thereafter.
The Ebola scare in the US exposed significant gaps in public health preparedness for highly contagious pathogens. It prompted substantial federal investments in biocontainment capabilities, rigorous screening of travelers from endemic areas at major airports, and revisions to hospital response protocols nationwide. While controversies arose concerning the adequacy of initial risk communication and the balance between humanitarian evacuations and border security measures, the overall outcome highlighted the adaptability and resilience of the US public health system in learning from immediate challenges. The sustained low risk of Ebola in the United States since 2016, despite subsequent outbreaks in the Democratic Republic of Congo and other African nations, reflects the enduring impact of these improved surveillance systems and geographic isolation.
Lasting Legacy and Lessons Learned from the 2014 Ebola Virus Epidemic
The 2014 West African Ebola epidemic left an indelible mark on global public health, serving as a stark reminder of the devastating potential of emerging infectious diseases. The human toll was immense, extending far beyond the immediate morbidity and mortality to include long-term health complications for survivors, socio-economic disruption, and psychological trauma for affected communities.
However, the crisis also spurred unprecedented international cooperation and innovation. It accelerated the development and deployment of rapid diagnostic tests, improved personal protective equipment, and, critically, paved the way for successful Ebola vaccines. The epidemic underscored several vital lessons:
- The Criticality of Public Health Infrastructure: Strong, resilient health systems at the local level are the first line of defense against outbreaks. This includes robust surveillance, diagnostic capabilities, and trained healthcare personnel.
- Importance of Community Engagement: Effective outbreak response relies heavily on building trust and working collaboratively with affected communities, respecting cultural norms while promoting safe practices.
- Rapid and Coordinated International Response: Global health security is a shared responsibility. Prompt, coordinated international aid, expertise, and resource allocation are essential to contain cross-border threats.
- Investment in Research and Development: The urgency of the 2014 crisis galvanized efforts to develop vaccines and therapeutics, proving that sustained investment in R&D is crucial for future pandemic preparedness.
- Enhanced Infection Control: Rigorous infection prevention and control protocols, especially in healthcare settings, are paramount to protecting healthcare workers and preventing nosocomial transmission.
Practical tips derived from the experience include the importance of early detection and isolation of cases, safe and dignified burial practices, comprehensive contact tracing, and sustained public health education campaigns. These measures are not merely theoretical but represent actionable advice for mitigating the impact of future outbreaks.
Conclusion
The 2014 West African Ebola epidemic was a watershed moment that reshaped global approaches to infectious disease outbreaks. While the journey was fraught with challenges and immense suffering, the lessons learned have fortified global public health preparedness, leading to more robust surveillance, swifter response mechanisms, and significant advancements in vaccine science. As new pathogens emerge and existing ones re-emerge, the enduring legacy of the 2014 Ebola virus crisis serves as a perpetual reminder of the need for constant vigilance, international solidarity, and unwavering commitment to global health security.