Ebola in the US: Navigating the 2014 Scare and Fortifying Public Health Preparedness
The year 2014 brought a novel and terrifying public health crisis to the forefront of American consciousness: the arrival of the Ebola virus on U.S. soil. While the West African Ebola epidemic raged abroad, infecting thousands, the confirmation of cases within the United States triggered widespread fear, intense media scrutiny, and a critical examination of the nation's ability to combat highly contagious pathogens. This period, marked by significant challenges and crucial lessons, ultimately galvanized efforts to enhance public health preparedness, transforming how the U.S. approaches infectious disease threats.
Understanding Ebola Virus Disease (EVD): The Invisible Threat
Ebola, formally known as Ebola virus disease (EVD) or Ebola hemorrhagic fever (EHF), is a severe and often fatal illness caused by one of four known ebolaviruses. This formidable pathogen is a zoonotic disease, meaning it originates in animals and can spill over into human populations. Fruit bats are considered the most likely natural reservoir for the
Ebola virus, with transmission to humans often occurring through contact with infected animals or their bodily fluids, particularly through practices like bushmeat hunting and consumption.
Once the virus crosses into humans, it spreads through direct contact with blood, secretions, organs, or other bodily fluids of infected people, and from contaminated surfaces and materials. Symptoms typically manifest anywhere from two days to three weeks post-infection, beginning insidiously with fever, profound fatigue, muscle pain, headaches, and a sore throat. As the disease progresses, these initial indicators give way to more severe symptoms, including vomiting, diarrhea, rashes, and impaired kidney and liver function. In advanced stages, internal and external bleeding can occur, making prompt diagnosis and isolation critical for both patient survival and preventing further transmission. The high mortality rate associated with EVD underscores the urgent need for robust public health responses.
The 2014 West African Ebola Epidemic: A Crisis Unfolding
The global context for the U.S. Ebola scare was the unprecedented 2014 West African Ebola epidemic, which marked the largest and deadliest outbreak of the disease in history. Originating in Guinea in December 2013, with the index case traced to a two-year-old child, the virus rapidly exploited weaknesses in health infrastructure and cultural practices to spread. By March 2014, the World Health Organization confirmed its presence, but the outbreak's momentum was already formidable.
Through cross-border travel and close family contacts, the
Ebola virus surged across Guinea, Liberia, and Sierra Leone. Nigeria also reported cases after a traveler from Liberia brought the virus to Lagos. This epidemic was characterized by fundamental failures in containment, including inadequate contact tracing, limited laboratory capacity for diagnosis, and healthcare systems overwhelmed by the sheer scale of the crisis. Ultimately, by June 2016, the epidemic had caused over 28,600 infections and claimed more than 11,300 lives across these nations, leaving a devastating legacy and serving as a stark reminder of the global interconnectedness of health threats. The sheer magnitude of this outbreak meant that it was only a matter of time before cases would appear in other parts of the world, including the United States.
Ebola in the US: The Dallas Cluster and a Nation on Edge
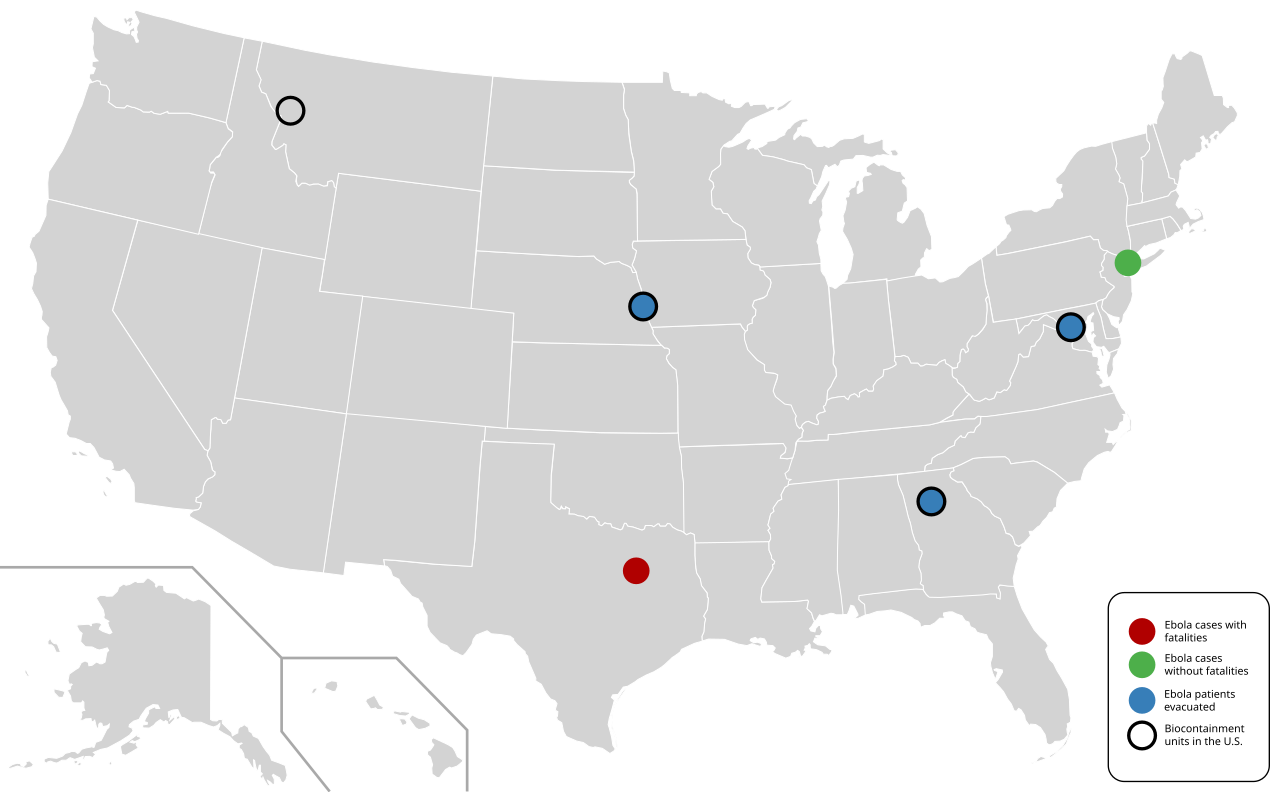
Between 2014 and 2016, the United States treated eleven individuals with confirmed Ebola virus disease. These cases were directly linked to the concurrent West African epidemic, primarily involving individuals who either contracted the virus abroad or healthcare workers who cared for them. The pivotal moment that ignited the U.S. public health scare was the case of Thomas Eric Duncan. An Liberian national, Duncan acquired the infection in his home country and traveled to Dallas, Texas, before becoming symptomatic. His initial presentation to a U.S. hospital was a critical failure point; despite reporting his recent travel from Liberia, he was initially misdiagnosed and sent home, only to return sicker days later.
Duncan's subsequent hospitalization at Texas Presbyterian Hospital resulted in two secondary transmissions to healthcare workers, nurses Nina Pham and Amber Vinson. These transmissions were a direct consequence of breaches in personal protective equipment (PPE) protocols and insufficient training for handling such a high-consequence pathogen. The "Dallas cluster" exposed significant vulnerabilities in U.S. hospital preparedness, from donning and doffing PPE to waste management and patient isolation.
Beyond the Dallas cluster, the remaining U.S. cases were primarily medical personnel or missionaries who had contracted the Ebola virus while working in affected regions of West Africa. These individuals were medically evacuated to the U.S. for treatment in highly specialized biocontainment units located at facilities such as the NIH Clinical Center in Maryland and Emory University Hospital in Georgia. These units, designed with stringent infection control measures, provided advanced supportive care and proved instrumental in the recovery of most patients. Tragically, Thomas Eric Duncan succumbed to the disease on October 8, 2014, and a physician infected abroad also passed away despite intensive treatment. However, critically, no further domestic transmissions occurred beyond the initial Dallas cluster, a testament to the rapid implementation of enhanced infection control measures.
Lessons Learned: Fortifying Public Health Preparedness for Future Threats
The 2014 Ebola scare, though contained, served as an invaluable, albeit difficult, stress test for the U.S. public health system. It exposed critical gaps in preparedness for highly contagious pathogens and catalyzed a sweeping overhaul of response protocols:
- Enhanced Infection Control and Biocontainment: The most immediate and significant change was a national focus on upgrading infection control capabilities. Hospitals across the country invested in rigorous training for healthcare workers on proper PPE use, waste disposal, and patient isolation. Federal investments poured into establishing and expanding specialized biocontainment units capable of safely managing highly infectious diseases, ensuring that future cases could be treated without risking widespread transmission.
- Robust Surveillance and Screening: Following the Dallas incident, the U.S. implemented enhanced screening protocols at major international airports for travelers arriving from Ebola-affected regions. This included temperature checks and health questionnaires, along with mandatory quarantines or active monitoring for individuals with potential exposure. This proactive approach aimed to detect and isolate cases before they could spread within communities.
- Improved Risk Communication: The initial phases of the outbreak saw controversies over the adequacy and clarity of risk communication from public health authorities. Lessons learned led to a renewed emphasis on clear, consistent, and transparent messaging to the public, aiming to mitigate fear while providing accurate information and actionable advice.
- National Coordinated Response: The crisis highlighted the need for a more unified and coordinated federal response. This led to better integration between federal agencies like the CDC and state/local health departments, streamlining communication and resource deployment during health emergencies.
- Global Health Security Investments: Recognizing that an outbreak anywhere can be a threat everywhere, the U.S. significantly increased its commitment to global health security initiatives. This included funding programs to strengthen health systems, surveillance capabilities, and rapid response teams in vulnerable countries, thereby tackling outbreaks at their source.
Despite subsequent outbreaks of the Ebola virus in the Democratic Republic of Congo and other African nations since 2016, no new cases have been reported in the United States. This sustained low risk reflects the effectiveness of the implemented measures, geographic isolation, and robust surveillance systems that continuously monitor global health threats. The episode also fueled debates on the balance between humanitarian evacuations for medical personnel and border security measures, highlighting the complex ethical and logistical challenges posed by such crises.
Conclusion
The 2014 Ebola scare in the U.S. stands as a pivotal moment in the history of American public health preparedness. While it exposed vulnerabilities and provoked widespread anxiety, it ultimately forged a stronger, more resilient system. The swift, decisive actions taken to enhance infection control, build biocontainment capabilities, and refine public health communication have created a robust framework for responding to future infectious disease threats. The experience underscored a fundamental truth: in an interconnected world, preparedness is not merely a domestic concern but a global imperative, demanding continuous vigilance, investment, and collaboration to safeguard public health and prevent a similar scare from becoming a larger catastrophe.